Navigating the Bones and Beyond: An Orthopaedic Roadmap

Send us a text Stepping into the world of orthopaedics can feel overwhelming. With musculoskeletal problems accounting for nearly a third of GP consultations, it's surprising that many medical professionals receive fewer than 60 hours of dedicated teaching in this crucial field. This episode offers a comprehensive framework for understanding orthopaedics—moving far beyond just "bones on x-rays" to explore how this specialty fundamentally improves quality of life. Dr. Gavin Nimon (Orthopaedic...
This is approved for 0.5 hour RACGP CPD - accredited activity
to complete - click on registration link after listenning
remember to provide RACGP member number and email
registration link
Stepping into the world of orthopaedics can feel overwhelming. With musculoskeletal problems accounting for nearly a third of GP consultations, it's surprising that many medical professionals receive fewer than 60 hours of dedicated teaching in this crucial field.
This episode offers a comprehensive framework for understanding orthopaedics—moving far beyond just "bones on x-rays" to explore how this specialty fundamentally improves quality of life. Dr. Gavin Nimon (Orthopaedic Surgeon) systematically breaks down the key symptoms that bring patients to orthopaedic care: pain (mechanical, inflammatory, traumatic, infectious, neoplastic, or neuropathic), stiffness (articular vs periarticular), deformity, swelling, weakness, instability, and neurological symptoms. Each presentation is explored with clarity, helping listeners develop a structured approach to diagnosis.
The episode introduces a valuable time-based lens for categorising presentations as acute, chronic, or mixed, guiding both urgency of intervention and management strategies. Gavin Nimon walks through the diagnostic pathway from clinical assessment to targeted investigations, emphasising the continued importance of plain radiographs alongside advanced imaging techniques. Particularly valuable is the discussion of orthopaedic emergencies that must never be missed—cauda equina syndrome, compartment syndrome, septic arthritis, open pelvic fractures, compound fractures, and acute septic flexor tenosynovitis—where early recognition can prevent devastating outcomes.
Whether you're a medical student, GP, or healthcare professional wanting to refresh your knowledge, this episode serves as an essential mental map of orthopaedics. Download the accompanying mind map from our website to reinforce these concepts and improve your approach to musculoskeletal conditions. Subscribe for more expert insights that bridge the gap between specialised knowledge and everyday clinical practice.
Aussie Med Ed is sponsored by -HealthShare is a digital health company, that provides solutions for patients, General Practitioners and Specialists across Australia.
Aussie Med Ed is sponsored by Avant Medical Indemnity: They state that they offer holistic support to help the doctor practice safely and believe they have extensive cover that's continually evolving to meet your needs in the ever changing regulatory environment.
00:47 - Introduction to Musculoskeletal Problems
02:39 - What is Orthopaedics?
03:23 - Diagnosing Through Symptoms: Pain
05:37 - Stiffness and Deformity
08:39 - Swelling, Weakness and Instability
12:33 - Neurological Symptoms and Congenital Conditions
18:40 - Acute vs Chronic Presentations
22:57 - Assessment, Teams and Emergencies
27:46 - Final Thoughts and Conclusion
WEBVTT
00:00:00.239 --> 00:00:02.189
Musculoskeletal problems are everywhere.
00:00:02.370 --> 00:00:10.679
They make up almost a third of GP consultations and yet study after studies show that medical students and even young doctors feel less confident in this area.
00:00:11.250 --> 00:00:20.219
Most of us get fewer than 60 hours of muscle-skeletal teaching in medical school, and a lot of that's just learning anatomy, but orthopaedics is so much more than bones on x-rays.
00:00:20.489 --> 00:00:24.329
It's about pain, stiffness, function, and more importantly, quality of life.
00:00:25.050 --> 00:00:28.440
In today's episode, we're gonna step back and look at the big picture.
00:00:28.875 --> 00:00:30.394
What actually is orthopaedics?
00:00:30.975 --> 00:00:34.365
How we make the diagnosis and the major ways patients present.
00:00:34.814 --> 00:00:40.274
We'll then touch on the wider team involved in the care and finish with the Orthopaedic emergencies that you must never miss.
00:00:40.814 --> 00:00:48.585
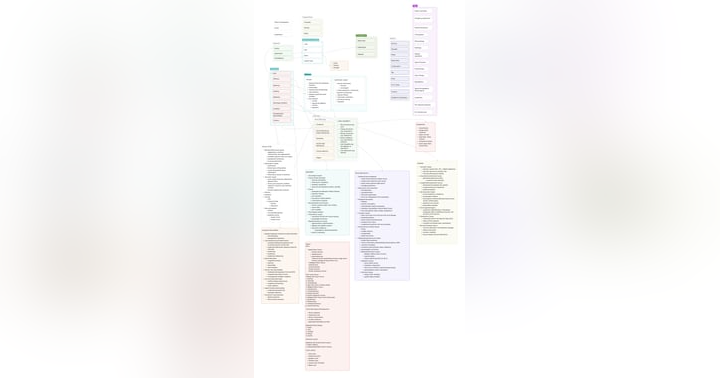
Think of this as a mind map of orthopaedics, a framework you can use whether you're a student, a gp, or just someone keen to understand better about this specialty.
00:00:49.274 --> 00:00:52.454
So let's grab a coffee and let's walk through the Orthopaedic mind map together.
00:00:54.225 --> 00:01:01.965
Good day and welcome to Aussie Med Ed, the Australian Medical Education Podcast designed with a pragmatic approach to medical conditions by interviewing specialists in the medical field.
00:01:02.564 --> 00:01:06.884
I'm Gavin Nimon, an Orthopaedic surgeon based in Adelaide, and I'm broadcasting from Kaurna Land.
00:01:07.575 --> 00:01:13.004
I'd like to remind you that this podcast is available on all podcast players as also available as a video version on YouTube.
00:01:13.784 --> 00:01:21.015
I'd also like to remind you that if you enjoy this podcast, please subscribe or leave a review or give us a thumbs up as I really appreciate the support and helps the channel grow.
00:01:21.555 --> 00:01:30.075
I'd like to start the podcast by acknowledging the traditional owners of the land on which this podcast is produced, the Kaurna people, and pay my respects, the elders, both past, present, and emerging.
00:01:34.484 --> 00:01:40.484
I'd like to remind you that all the information presented today is just one opinion, and that there are numerous ways of treating all medical conditions.
00:01:40.963 --> 00:01:45.134
It's just general advice and may vary depending on the region in which you are practicing or being treated.
00:01:45.853 --> 00:01:52.664
The information may not be appropriate for your situation or health condition, and you should always seek the advice from a health professional in the area in which you live.
00:01:52.844 --> 00:01:53.804
What is orthopaedics?
00:01:54.284 --> 00:01:59.689
Well, orthopaedics deals with musculoskeletal system, bones, joints, muscles, ligaments, tendons and nerves.
00:02:00.420 --> 00:02:03.480
But it's not just about the bones, it's about function and movement.
00:02:03.870 --> 00:02:15.090
It's about restoring quality of a life, whether you're a tradie, getting back on the site after a fracture, an athlete returning to play after a ligament injury, or an older person wanting to walk pain free to the shops.
00:02:15.479 --> 00:02:16.680
That's what we look after.
00:02:17.250 --> 00:02:27.509
We see patients across the entire lifespan from newborns with congenital problems to elderly patients with arthritis and fractures, and importantly, Orthopaedic surgeons aren't only just surgeons.
00:02:27.780 --> 00:02:34.199
Sometimes we operate, yes, but often we manage conditions conservatively with therapy, rehab, or even injections.
00:02:35.639 --> 00:02:37.259
So let's start with diagnosis.
00:02:37.289 --> 00:02:42.000
Well, the way we diagnose it always starts with a history, the story the patient tells us.
00:02:42.180 --> 00:02:48.030
And that story is usually built around symptoms that's goes through those key symptoms categories one by one.
00:02:48.539 --> 00:03:02.308
Remember, the diagnosis is often what makes the history or the examination helps us confirm the diagnosis and the investigations while adding to the diagnosis confirmation, they can be used for staging So as determine treatment options and determine prognosis.
00:03:03.629 --> 00:03:06.659
So the first symptoms that patients may present with is pain.
00:03:07.049 --> 00:03:13.649
It's most common reason patients see us, but not all pains are equal Mechanical pain is a pain of wear and tear.
00:03:14.159 --> 00:03:16.709
Think of osteoarthritis or disc degeneration.
00:03:17.069 --> 00:03:19.704
It worsens with activity and it settles with rest.
00:03:20.084 --> 00:03:26.479
It can also come on from instability, like a torn ligament or from impingement syndromes in the shoulder or in the hip.
00:03:27.560 --> 00:03:29.750
Inflammatory pain is somewhat different.
00:03:30.050 --> 00:03:31.460
This is worse in the morning.
00:03:31.490 --> 00:03:36.560
Often with stiffness lasting more than half an hour and improves as the patient gets moving.
00:03:37.069 --> 00:03:44.990
It's typical of autoimmune and inflammatory arthropathies, but also crystal arthritis like gout and shadow gout, or even inflammatory tendonitis and bursitis.
00:03:46.099 --> 00:03:59.360
Traumatic pain is either from acute can be either acute from fractures, dislocations, or ligament injuries, or chronic from poorly healed fractures, malunion, non-unions, or even getting post-traumatic arthritis.
00:03:59.900 --> 00:04:03.229
In some cases, it progresses to complex regional pain syndrome.
00:04:03.740 --> 00:04:06.020
This is where the pain is outta proportion to the injury.
00:04:07.639 --> 00:04:09.889
Infection is always on the list of causing pain.
00:04:10.400 --> 00:04:13.189
Septic arthritis or osteomyelitis can present with acute pain.
00:04:13.775 --> 00:04:22.355
And with systemic illness as well, whilst neoplasms, they can cause deep, unrelenting, often night pain, not relieved by rest.
00:04:23.134 --> 00:04:26.165
Nerve entrapment, however, is often a good cause of pain.
00:04:26.464 --> 00:04:28.805
And that's a burning, shooting, electric type pain.
00:04:28.915 --> 00:04:38.995
and with classic examples being things like sciatica or cervical radiculopathy, very painful conditions, or even peripheral nerve entrapments, like carpal tunnel, cubital tunnel syndromes.
00:04:39.985 --> 00:04:42.954
So when a patient says, look, doc, I've got a lot of pain.
00:04:43.314 --> 00:04:46.795
We are already sorting through one of these sort of categories when we're assessing the patient.
00:04:46.875 --> 00:04:49.545
Stiffness, however, can be just as disabling as pain.
00:04:49.964 --> 00:04:55.214
We can split this into articular causes, stiffness or Periarticular causes stiffness.
00:04:55.394 --> 00:04:59.415
Secondary to articular causes is that stiffness that occurs from within inside the joint.
00:05:00.105 --> 00:05:22.600
The most common one is being osteoarthritis with the bony spurs and the loose body's jamming in the joint, but also with the capsular tightness that occurs around the joint associated with this Meniscal tears can also cause a locking type sensation in the knee, for instance, and that can cause stiffness, secondary to a locked knee, whilst fluid in the knee with big effusions can cause filling of the joint and therefore stiffness.
00:05:22.600 --> 00:05:29.591
Secondary to that, and one of the most common causes of an intraarticular stiffness is the adhesive capsulitis or frozen shoulder.
00:05:29.935 --> 00:05:33.505
With stiffness associated with that, usually presenting after severe pain.
00:05:34.675 --> 00:05:39.266
Post infective arthritis is another cause of stiffness where the joint gets scarred and bound down.
00:05:40.586 --> 00:05:43.406
periarticular causes, however, come from outside the joint.
00:05:43.766 --> 00:05:47.875
These are muscle contracture, either from scarring or from neurological conditions.
00:05:48.206 --> 00:05:52.600
,Often in the case, tendon adhesions or shortening can also lead to stiffness.
00:05:53.350 --> 00:06:06.680
As can ligament contractures and capsular fibrosis, as said before, is probably one of the most common causes with osteoarthritis, causing both the intraarticular stiffness as well as a capsular, almost extra-articular element to it as well.
00:06:08.990 --> 00:06:22.610
Heterotopic ossification after head trauma or after a significant bleed can also lead to stiffness where bone is formed where it shouldn't be developing, and soft tissue scarring around a joint can also lead to stiffness also.
00:06:23.779 --> 00:06:27.480
And even soft tissue tumours pressing on a joint can cause the symptoms of stiffness.
00:06:27.870 --> 00:06:31.800
So stiffness isn't just stiffness, it's a whole spectrum of underlying pathology.
00:06:32.550 --> 00:06:35.189
A third symptom the patient can present with is deformity.
00:06:35.699 --> 00:06:40.920
This can be dramatic or subtle, and again, we've gotta think about articular versus periarticular causes.
00:06:41.579 --> 00:06:48.389
Articular causes include osteoarthritis once again with either particularly in the knee, causing a varus or valgus deformity.
00:06:48.509 --> 00:06:50.250
In other words, a bow in or bows out.
00:06:50.925 --> 00:07:01.694
But fractures that heal crooked or in an abnormal plane can lead to deformity such as a distal radial fracture with dorsal angulation can lead to a classic thin fork deformity.
00:07:02.264 --> 00:07:13.560
And also congenital deformities can occur like club foot or hip dysplasia or the hip also infection destroying a joint or tumours distorting a joint or bone can lead to deformity.
00:07:15.290 --> 00:07:32.124
Periarticular causes are are causes that occur around the soft tissues, around the joint or bone and muscle contractures from scarring or neurological disease can lead to tendon shortening or adhesions, ligament contractures, capsular fibrosis, and again, that can lead to deformity.
00:07:33.038 --> 00:07:38.678
So really the question is always is, is the deformity coming from the bone, the joint, or the soft tissues around it?
00:07:38.709 --> 00:07:42.338
One of those three structures, again, obeying the rule of threes.
00:07:43.338 --> 00:07:47.119
Swelling, is another common complaint, and the cause of this are many.
00:07:47.559 --> 00:07:57.262
most the swellings we see are traumatic and associated with fractures or soft tissue sprains, ligament injuries, contusions, or even dislocations if they're quite deformed.
00:07:58.523 --> 00:08:01.432
But you can get inflammation inside of joint causing swelling.
00:08:01.793 --> 00:08:12.682
And the classic causes of arthritis, either osteoarthritis or the inflammatory arthritis can cause swelling themselves along with crystalline depositions such as gout or shooter gout.
00:08:13.372 --> 00:08:18.023
And again, we've always gotta remember infection, septic, arthritis being a major issue.
00:08:18.432 --> 00:08:27.158
So if someone's presenting with acute, painful, swollen joint Septic arthritis needs to be excluded, and soft tissue swelling around the joint, but not involving the joint.
00:08:27.158 --> 00:08:32.437
Could be from a cellulitis or an abscess, or even a bursitis, either septic or aseptic.
00:08:34.298 --> 00:08:37.837
There are other causes of swelling though that aren't quite classic of orthopaedics.
00:08:38.138 --> 00:08:41.107
You gotta think of things like deep vein thrombosis or lymphoedema.
00:08:41.408 --> 00:08:50.712
And of course, in an acute traumatic scenario such as a fractured Tibia, you gotta think of a swollen leg secondary to trauma, which can have an associated compartment syndrome.
00:08:51.482 --> 00:08:56.635
Slowly progressing s welling can be caused by a soft tissue or bone tumours as well.
00:08:57.056 --> 00:09:03.475
And generalized swelling considered, heart failure or renal or liver disease can cause a scenario with that.
00:09:04.946 --> 00:09:12.206
Always if someone develops swelling suddenly, particularly after they've being given a medication, you always gotta think of an allergic or immunological response.
00:09:13.346 --> 00:09:21.446
So really the timing and distribution of the swelling really helps affect or determine what the diagnosis is and needs to be taken into account.
00:09:21.566 --> 00:09:25.846
The next presentation might be something like weakness, and this can be either genuine or apparent.
00:09:26.596 --> 00:09:29.716
The most common cause of weakness might relate to neurological disorders.
00:09:29.716 --> 00:09:31.846
Such as an upper motor neuron disease, and a stroke.
00:09:32.355 --> 00:09:37.395
Or spinal cord injury are probably the most serious scenarios in that situation.
00:09:37.666 --> 00:09:45.285
But you can get peripheral neuropathies leading to a muscular or a radiculopathy leading to weakness or even motor neuron disease.
00:09:46.155 --> 00:09:56.296
Again, you gotta think of other general symptoms like primary muscular disorders, muscular dystrophies or metabolic myopathies or drug induced myopathies could be a factor of weakness.
00:09:57.301 --> 00:10:03.780
But probably in orthopaedics, one of the most common things that we would see for leading to weakness is disuse.
00:10:04.051 --> 00:10:24.331
And that might be, that might be secondary immobilization, either primarily caused by the use of a plaster to immobilize a limb whilst the bone is healing, or in the period after say shoulder surgery and then being placed in a sling or could be secondary to the pain that's been caused by an Orthopaedic condition leading to generalized weakness or muscle wasting.
00:10:24.811 --> 00:10:27.030
But you also get it in postoperative surgery.
00:10:27.091 --> 00:10:31.201
You can get weakness and in the elderly you get sarcopenia, which can lead to weakness.
00:10:32.041 --> 00:10:51.890
Weakness can actually be secondary to loss of the actual motor power of the joint, and that can be either secondary to nerves as we've outlined above, but also, you gotta remember , acute tendon ruptures can lead to weakness as can, obviously joint instability, where they get sensational, the joint's going to subluxate or dislocate, and therefore they have a inhibition of movement.
00:10:52.671 --> 00:10:53.931
This also occurs in pain.
00:10:53.931 --> 00:11:04.250
When someone's got a pain around a joint, they don't like to push through it because it hurts and of, cause anything that causes inflammation, causes weakness as well, secondary to the pain in that scenario.
00:11:05.061 --> 00:11:09.530
Finally, you gotta think about things like metabolic causes and endocrine causes causing weakness.
00:11:09.831 --> 00:11:14.421
Such as thyroid disease or diabetes, or even electrolyte imbalances.
00:11:14.750 --> 00:11:17.900
So sorting through true weakness and power weakness is important.
00:11:18.860 --> 00:11:19.971
As an upper limb surgery.
00:11:19.971 --> 00:11:22.910
One of the more common reasons a patient might present to me is from instability.
00:11:23.331 --> 00:11:25.130
Instability is not that hard to diagnose.
00:11:25.130 --> 00:11:29.270
'cause often the patient feels like the shoulder or the joint they're talking about pops out a joint.
00:11:29.630 --> 00:11:31.910
They feel that it gives way or feels unstable.
00:11:32.571 --> 00:11:35.120
These traumatic causes are the most common scenarios where.
00:11:35.490 --> 00:11:42.931
As a joint is subjected to trauma, the ligaments disrupt around it and in the shoulders, the labrum actually tears, which is the thickening of the capsule.
00:11:43.740 --> 00:11:51.181
But you also, you can get a traumatic cause of instability, and this can be related to constitutional causes, such as patients with generalized ligament laxity.
00:11:51.181 --> 00:11:54.841
Therefore, they've got a multi-directional instability, for instance.
00:11:55.110 --> 00:11:57.780
Or they may have connective tissue disorders as well as part of this.
00:11:58.530 --> 00:12:12.581
There are congenital causes as well, and one of the more common ones I think about is developmental dysplasia of the hip, where the newborn needs to be assessed to make sure the hip feels stable and if not needs to be immobilized so that the, the acetabulum develops around it.
00:12:13.421 --> 00:12:18.865
There are also skeletal dysplasias can lead to deformities of the joints and therefore instability.
00:12:20.485 --> 00:12:25.826
Neuromuscular causes are another cause to think about with muscle weakness and poor proprioception.
00:12:26.143 --> 00:12:34.452
muscle contractures or even peripheral nerve injuries lead to slowly deforming joints and therefore a chronic type instability.
00:12:36.038 --> 00:12:40.839
And then again, after surgery, even including hip replacements, these joints can dislocate.
00:12:42.894 --> 00:12:48.653
Associated with rheumatoid arthritis and other inflammatory arthropathies, as well as crystalline arthropathies like gout.
00:12:48.953 --> 00:12:52.884
You can get stretching of the capsules, destruction of the joints and the ligaments around it.
00:12:53.214 --> 00:12:58.283
Leading to instabilities and in the rheumatoid disease is very common in the metacarpal phalangeal joints.
00:12:59.484 --> 00:13:07.764
Now, one of the lesser causes or presentations to an Orthopaedic surgeon might be from neurological sensory deficit, but it's not that unusual in an upper limb surgeon.
00:13:08.168 --> 00:13:13.958
Where we'll see symptoms of paraesthesia and numbness or weakness in one of the nerves in the upper limb.
00:13:13.958 --> 00:13:17.048
The classic one being the carpal tunnel or cubital tunnel syndrome.
00:13:17.318 --> 00:13:26.109
You can get in leg as well around the upper thigh called Meralgia Paraesthetica where the lateral cutaneous nerve of the thigh gets trapped or tarsal tunnel syndrome.
00:13:27.548 --> 00:13:35.563
Probably even more common than that is spinal root issues such as a disc prolapse secondary or secondary to a spondylothesis or secondary to.
00:13:36.249 --> 00:13:42.436
Degenerative arthritis and that's pressing on the spinal nerve roots that can cause a severe shooting pain down the leg.
00:13:42.645 --> 00:13:57.176
You always must remember though, when you see these neurological conditions that the peripheral neuropathies can be general as well, and the most common what scenario nowadays is diabetes with the high sugar levels causing primary nerve damage.
00:13:57.416 --> 00:13:59.513
But you can also get a second to medications.
00:13:59.842 --> 00:14:02.873
Particularly chemotherapy agents as well as alcohol.
00:14:03.322 --> 00:14:08.842
And there are also hereditary causes where patients are more prone to nerve entrapments in general.
00:14:10.493 --> 00:14:20.125
Finally, traumatic scenarios can occur after direct trauma to the nerve, , such as a stabbing or brachial plexus trauma stretching the nerves.
00:14:20.410 --> 00:14:28.030
. There's also iatrogenic causes that can occur and post-surgery as well as the risk of compartments syndrome lead to secondary nerve damage.
00:14:28.931 --> 00:14:29.480
In orthopaedics.
00:14:29.500 --> 00:14:38.221
Two, though we must always remember other medical type causes such as stroke, multiple sclerosis, and spinal cord tumours aren't outta the question as well.
00:14:38.941 --> 00:14:41.791
And then there's unfortunately, we've gotta keep in mind open to.
00:14:42.211 --> 00:14:51.421
Rarer, but important scenarios such as the autoimmune type or inflammatory type conditions such as Guillane-Barre, or vascular neuropathy, et cetera.
00:14:52.500 --> 00:15:04.476
So there's lots of causes of nerve issues to be aware of and, , we need to take those into account when assessing our patients with a presentation with muscle weakness or sensory issues and presenting with a neurological type of thing.
00:15:05.596 --> 00:15:06.586
We always gotta remember.
00:15:06.586 --> 00:15:19.260
However, after spinal injury, don't forget the significant and very important scenario of Cauda-Equina syndrome, which can present with subtle reduction of perianal sensation and loss of urinary or bowel movements.
00:15:19.441 --> 00:15:23.850
And this can occur from a significant disc prolapse pushing on the spinal nerve roots.
00:15:24.390 --> 00:15:33.811
Now, moving along to other symptoms a patient may present with, well, congenital abnormalities are not uncommon to the group of pediatric Orthopaedic surgeons.
00:15:34.140 --> 00:15:36.030
They bring their own spectrum of conditions.
00:15:36.030 --> 00:15:37.681
You gotta think of skeletal dysplasias.
00:15:38.410 --> 00:15:48.285
Achondroplasia, osteogenesis imperfecta can present in various presentations or growth abnormalities, and you also can get limb deficiencies of the transverse or longitudinal.
00:15:48.706 --> 00:16:01.576
And when it comes to the spine, you also can get issues such as spina bifida, or hemi vertebrae, along with foot and ankle deformities, such as club feet, tarsal coalitions, and scenarios like Sprengel's deformity.
00:16:03.135 --> 00:16:07.635
Along with all these things, you can get these connective tissue disorders, which we've touched about before.
00:16:07.865 --> 00:16:10.456
Ehlers-Danlos or Marfan's syndromes as well.
00:16:11.145 --> 00:16:22.846
So these congenital abnormalities is a extra element to orthopaedics treatment, which is managed usually by specialist pediatric Orthopaedic surgeons who specialize in these areas primarily.
00:16:23.086 --> 00:16:27.525
But in a general scenario, a lot of Orthopaedic surgeon will have some experience with these as well.
00:16:28.336 --> 00:16:30.346
That brings me on to my final reason.
00:16:30.346 --> 00:16:31.515
A patient may present.
00:16:32.010 --> 00:16:39.160
To an Orthopaedic surgeon is with a lump, and these can be what I would describe as tumours and bone or soft tissue lesions.
00:16:39.581 --> 00:16:55.630
These can be divided up into benign bone tumours such as osteoid osteoma or osteoblastoma or enchondroma Which often are incidental findings on, on x-rays or malignant bone tumours such as osteosarcoma or chondrosarcoma or primary lymphoma of bone.
00:16:57.071 --> 00:17:04.000
We can also get soft tissue benign lesions such as lipomas, a lump in the fat, which develops in the soft tissues and presents as a lump.
00:17:04.601 --> 00:17:06.671
You get giant cell tumours or tendon sheaths.
00:17:07.121 --> 00:17:13.121
We get malignant soft tissue tumours such as lipomas, synovial sarcomas, et cetera.
00:17:13.421 --> 00:17:15.131
And then there's tumor like lesions.
00:17:15.476 --> 00:17:33.526
Bone cysts and metastatic disease, which is the secondary cancers that have spread to the bone, breast, lung, prostate, kidney, and thyroid, and finishing off systemic lesions like Paghet's disease or hyperparathyroidism can present with bone deformities or lumps.
00:17:34.996 --> 00:17:39.306
One really useful way of thinking about Orthopaedic problems also is, is to apply a surgical sieve.
00:17:40.006 --> 00:17:44.355
Breaking these conditions down into acute, chronic, and mixed presentations.
00:17:44.355 --> 00:17:47.086
This is the thing I really emphasize when I'm teaching.
00:17:47.596 --> 00:17:53.655
It doesn't replace these categories and how patients present, but instead it gives you a time-based lens to look through.
00:17:54.705 --> 00:17:58.455
So if you look at acute presentations, these are sudden onset, often dramatic.
00:17:58.695 --> 00:18:04.665
There are the classic reasons people turn up to the emergency department or to their GP with something they can't ignore.
00:18:05.445 --> 00:18:07.118
Well, if you look, at the traumatic causes.
00:18:08.034 --> 00:18:19.044
Fractures, dislocations, acute ligament ruptures, tendon tears or meniscal injuries really fit into this area, but you , can't forget things like infections such as septic arthritis.
00:18:19.493 --> 00:18:22.673
The key to this group is the acute problems present with urgency.
00:18:23.124 --> 00:18:28.314
The diagnosis may not be difficult to make, but the priority is acting quickly to prevent long-term disability.
00:18:28.898 --> 00:18:30.219
Chronic presentations.
00:18:30.638 --> 00:18:35.368
These are things that a patient might present to a GP or a Orthopaedic clinic.
00:18:35.368 --> 00:18:45.659
For degenerative conditions like arthritis or degenerative disc disease or rotator cuff degeneration really are the main treat conditions that present in this scenario.
00:18:46.048 --> 00:18:47.219
They present with gradual pain.
00:18:47.219 --> 00:18:50.999
They may present with stiffness and they may present with deformity.
00:18:52.064 --> 00:19:00.463
Inflammatory disorders such as rheumatoid arthritis gout, ankylosing spondylitis can, uh, can also come on suddenly.
00:19:00.463 --> 00:19:04.993
They might have a flare up, but they usually are slowly progressing well with intermittent flare ups.
00:19:07.094 --> 00:19:16.364
Chronic conditions rarely require emergency intervention, but essential to what we do in orthopaedics, s restoring movement, correcting deformity, and preserving independence.
00:19:17.054 --> 00:19:19.693
But amongst acute and chronic presentations, you get a mixed picture.
00:19:20.503 --> 00:19:25.034
This is where things overlap, where longstanding conditions suddenly tips into an acute event.
00:19:25.604 --> 00:19:30.614
These are often the most challenging because you have to deal with both the underlying pathology and the new complication.
00:19:31.544 --> 00:19:45.374
They're not that common, but scenarios might be a patient with osteoarthritis who suddenly develops a locked knee secondary to a loose fragment sitting inside the knee joint, or there might be a metabolic bone disorder, which suddenly leads to develop some malignancy.
00:19:47.023 --> 00:19:58.856
Or there may be avascular necrosis, which suddenly it's been simmering along for years, but suddenly collapses, secondary to the loss of, bone structure leading to acute pain, and then development of secondary arthritis.
00:19:59.817 --> 00:20:05.876
Even congenital deformities such as scoliosis can sudden accelerate or decompensate during growth spurts.
00:20:06.717 --> 00:20:14.291
So mixed cases remind us that timeframes can overlap and the patient may live with a condition for years, but the reason they seek help is the acute change that just occurred.
00:20:15.852 --> 00:20:27.971
So when you're faced with a new patient, you can think not just about the symptom, you know, the pain, the stiffness, the deformity, the swelling, the weakness, the instability or neurological problem, but also what time course it was.
00:20:27.971 --> 00:20:29.622
Is it acute or is it chronic?
00:20:30.791 --> 00:20:39.372
This mental framework helps you triage urgency, choose investigations and decide whether the problem is one for the emergency department or an Orthopaedic outpatient.
00:20:41.501 --> 00:20:56.676
Once we've done a assessment, looking into both their history and how they presented and the symptoms they presented with, we can go to examination and in that process we go down the path of the look, feel, move, and special test approach.
00:20:57.217 --> 00:20:58.836
We always look at posture.
00:20:58.836 --> 00:21:01.326
We look for scars and wasting and deformity.
00:21:01.626 --> 00:21:05.946
We feel for warmth around the joint and we look for tenderness and swelling around the joint.
00:21:06.041 --> 00:21:07.332
We move the joint.
00:21:07.392 --> 00:21:11.922
We start with active motion and assist it with passive to see if that's greater.
00:21:12.192 --> 00:21:17.021
And then we use special tests to confirm our suspicions of what the diagnosis might be.
00:21:18.162 --> 00:21:20.142
Investigations are what follow after that.
00:21:20.622 --> 00:21:22.692
These help support our clinical impression.
00:21:23.592 --> 00:21:24.971
Don't forget bloods.
00:21:25.122 --> 00:21:30.491
We can check bloods looking for infection, inflammation, or metabolic disease, and then we proceed to imaging.
00:21:31.092 --> 00:21:33.402
I like to always think of plain x-rays first.
00:21:34.227 --> 00:21:44.217
You always want to consider and get so much information about a plain X-ray that they should not never be excluded unless it's, unless a particularly rare situation where it's not required.
00:21:44.817 --> 00:21:48.836
We then can use move to ultrasound, CT or MRI, depending on the problem.
00:21:49.406 --> 00:21:55.196
And of course up our sleeve we've got things like biopsies if we're worried particularly about a tumor or an unexplained lesion.
00:21:55.467 --> 00:21:59.636
Although nowadays a lot of these biopsies are done by dedicated tumour services.
00:22:00.416 --> 00:22:02.866
And that brings me up to the subdivision of orthopaedics.
00:22:03.517 --> 00:22:18.656
orthopaedics today is becoming more highly specialized by region, spine, shoulder, elbow, hand, hip, knee, foot, ankle, and by patient group, pediatrics or adult or by or condition tumour or trauma or deformity correction.
00:22:19.737 --> 00:22:22.886
And this is not just the Orthopaedic surgeon, of course it's a team.
00:22:23.126 --> 00:22:25.826
Remember, Orthopaedic is a team effort around the surgeon.
00:22:25.826 --> 00:22:26.636
There is anesthetists.
00:22:26.636 --> 00:22:28.301
There's rheumatologists, radiologists.
00:22:28.916 --> 00:22:36.446
Sports physician physiotherapists, occupational therapists, rehab specialists, and sometimes neurosurgeons or oncologists.
00:22:36.987 --> 00:22:47.457
And at the center, of course, it's always the patient and their family, and also directed and orchestrated by the referring doctor, the general practitioner or the emergency department, where it's a two way street.
00:22:47.916 --> 00:22:50.152
Finally Let's move on to the Orthopaedic emergency we should never, miss.
00:22:51.311 --> 00:23:03.701
Probably the most important one is a Cauda-equina syndrome where back pain, uh, secondary to a large disc prolapse presses on the sacral nerve roots and can lead to urinary or bowel involvement, and does require urgent decompression.
00:23:04.511 --> 00:23:13.961
Compartment syndrome where the pain's out of proportion after a traumatic incident, this compartment swells up with fluid, puts pressure on the vessels feeding that compartment.
00:23:14.576 --> 00:23:22.707
Reducing the circulation to that compartment, leading to increasing muscle damage and lead to secondary, more pressure on the compartment.
00:23:23.037 --> 00:23:24.807
This requires urgent fasciotomy.
00:23:25.586 --> 00:23:26.997
Septic arthritis.
00:23:27.477 --> 00:23:34.076
As I said before, hot, swollen, painful joint will require surgical washout and antibiotics.
00:23:34.076 --> 00:23:38.142
If not treated, it can lead to secondary arthritis and then lead to stiffness.
00:23:39.176 --> 00:23:51.767
And open book fractures where the pelvis has been damaged, such that the pubic symphysis or the pubic rami, along with the -sacral joints are damaged such that the whole pelvis splays open.
00:23:52.217 --> 00:24:03.761
This can lead to catastrophic blood loss, needing urgent stabilization, and can be easily initially treated by pelvic binding, but often will require surgery such as plating or an external fixator.
00:24:04.067 --> 00:24:14.386
And then of course there's things like compound fracture, open fracture, where the bone is sticking out through the soft tissues and requires antibiotic debridement reduction and stabilization.
00:24:14.866 --> 00:24:25.497
And the one that a lot of people, aren't aware of is acute septic flexor tenosynovitis, where an infection in the tendon sheath in the hand leads to a localized compartment syndrome, as well as a lot of scarring.
00:24:25.797 --> 00:24:29.846
And if left can lead to severe damage, then it requires surgical drainage.
00:24:30.356 --> 00:24:31.707
These are all time critical.
00:24:32.247 --> 00:24:35.487
Recognizing them early, acting fast upon them can affect the outcome.
00:24:35.636 --> 00:24:56.211
So that's the Orthopaedic framework from how our patient presents from pain, stiffness, deformity, swelling, weakness, instability, neurological symptoms, congenital conditions or lesions can help us, guide us where we proceed with our examination investigations and which team are involved, as well as knowing how they present too.
00:24:56.281 --> 00:25:00.537
They present the acute or traumatic event offers a combination of the two.
00:25:01.092 --> 00:25:10.271
Combining these and assessing a patient, knowing the conditions can that develop, and being aware of what help you've got around can really help guide you.
00:25:10.571 --> 00:25:22.001
And that's why knowing about the teamwork that makes up an Orthopaedic team and also the emergencies not to miss, hopefully this gives you a little bit of information to take away and keep in the back of your mind.
00:25:22.241 --> 00:25:29.352
So if you take nothing else away, remember this orthopaedics is about restoring movement and function and emergencies must never be ignored.
00:25:30.041 --> 00:25:32.291
Once again, thank you very much for listening to this podcast.
00:25:32.291 --> 00:25:33.432
I really hope you've enjoyed it.
00:25:33.582 --> 00:25:42.251
I've actually enclosed a mind map, which is attached to the website if you'd like to look at it, and is also on the YouTube channel as well.
00:25:43.031 --> 00:25:46.811
Thanks again for listening to the podcast and please subscribe to the podcast for the next episode.
00:25:47.261 --> 00:25:49.182
Until then, please stay safe.